CHEST Releases Guideline on Management of Early-Stage Non-Small Cell Lung Cancer
July 28, 2025
Glenview, Illinois –The American College of Chest Physicians® (CHEST) recently released a new clinical guideline on the management of patients with early-stage non-small cell lung cancer (NSCLC). Published in the journal CHEST®, the guideline contains 17 evidence-based recommendations to provide a framework for clinicians to implement in their own practice.
Lung cancer remains the number one cause of cancer death in men and women in the United States and much of the world. This CHEST guideline examines the literature on primary treatment of patients with stage I and II NSCLC to provide evidence-based recommendations.
“As with the release of any new guideline, our goal is to help standardize the approach to treatment and management of care,” said John Howington, MD, MBA, FCCP, 2025 President of CHEST and lead author on the guideline. “Variable care is often associated with lower quality care, and guidelines are a great way to share best practices far and wide to improve patient outcomes.”
The panel applied the Grading of Recommendations, Assessment, Development, and Evaluations approach to assess the certainty of evidence and to formulate and grade recommendations. They also created three flowchart graphs outlining the recommended course of treatment: one for patients who are medically inoperable, one for patients with high-operative risk, and one for patients with average risk.
“In the time since the last guideline on this topic was published by CHEST, there have been several landmark trials that have taught us a lot about treating early-stage lung cancer,” said Dr. Howington. “As an example, we knew that there were short-term benefits to minimally invasive surgeries because of shorter hospital stays, less pain, and the like, but now we have the evidence to show that minimally invasive surgery for stage I lung cancer is also associated with better long-term survival.”
Of the 17 recommendations, highlights include:
- In patients with clinical stage I NSCLC, we recommend minimally invasive approaches over thoracotomy.
- For patients with completely resected stage II NSCLC, we recommend treatment with adjuvant chemotherapy.
- For patients with resected stage IB NSCLC and epidermal growth factor receptor ex19del/L858R mutations, we recommend treatment with adjuvant targeted therapy.
- In medically fit patients with a peripheral ≤ 2 cm solid or mostly solid clinical stage I NSCLC, we suggest either lobectomy, segmentectomy, or sublobar nonanatomic (wedge) resection as equivalent alternatives.
The entire list of recommendations included in the new guideline can be accessed through the CHEST journal website in the article titled, “Management of Patients with Early-Stage Non-Small Cell Lung Cancer: An American College of Chest Physicians Clinical Practice Guideline.”
About the American College of Chest Physicians
The American College of Chest Physicians® (CHEST) is the global leader in the prevention, diagnosis, and treatment of chest diseases. Its mission is to champion advanced clinical practice, education, communication, and research in chest medicine. It serves as an essential connection to clinical knowledge and resources for its 18,000+ members from around the world who provide patient care in pulmonary, critical care, and sleep medicine. For information about the American College of Chest Physicians and its family of journals, including the flagship journal CHEST®, visit chestnet.org.
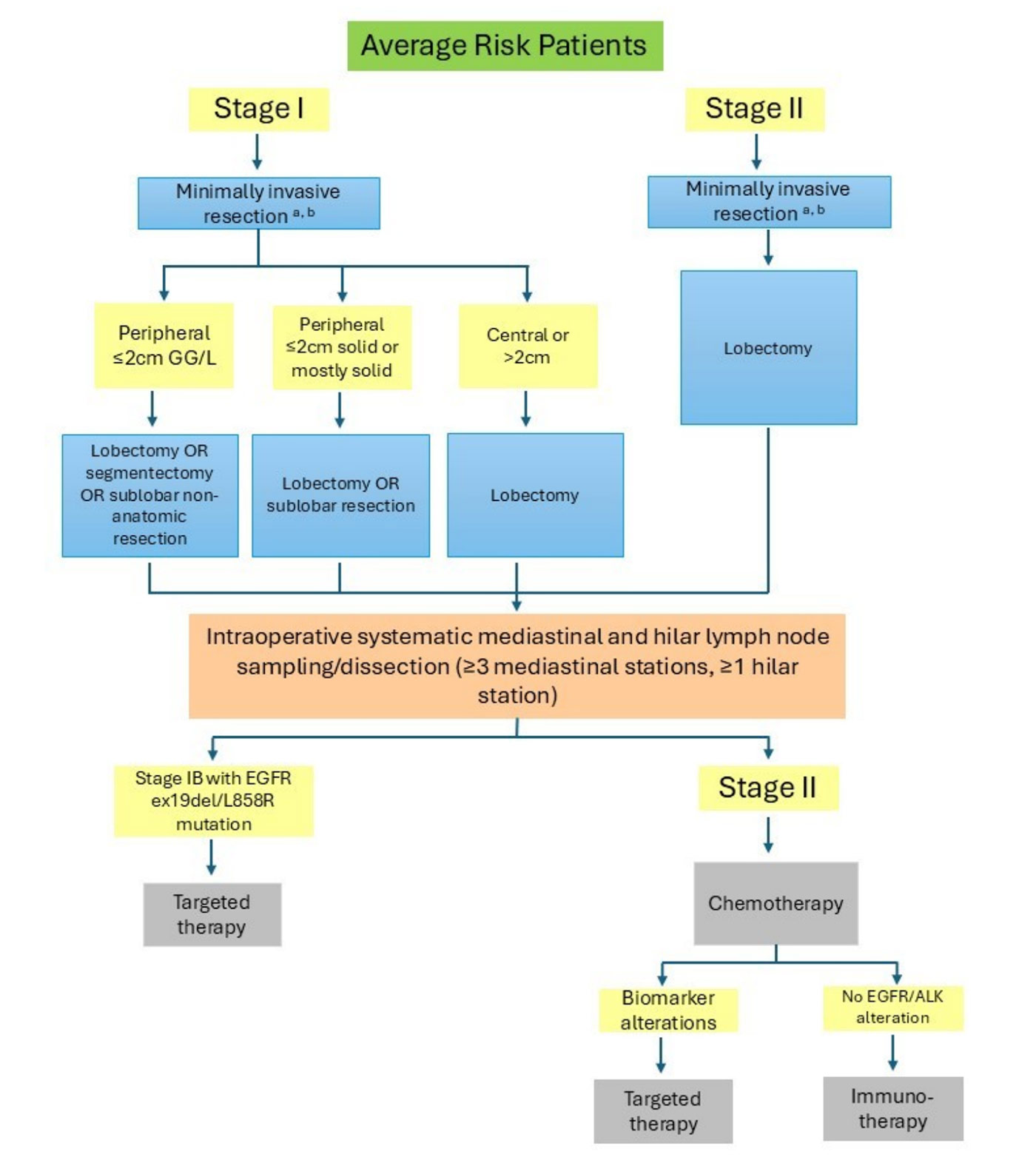 Figure 1 Sample management algorithm for average-risk patients.
Figure 1 Sample management algorithm for average-risk patients.
A. Resection suggested over stereotactic body radiotherapy or ablative techniques.
B. Resection by a board-certified thoracic surgeon suggested.
ALK = anaplastic lymphoma kinase; EGFR = epidermal growth factor receptor; GG/L = ground-glass/lepidic.
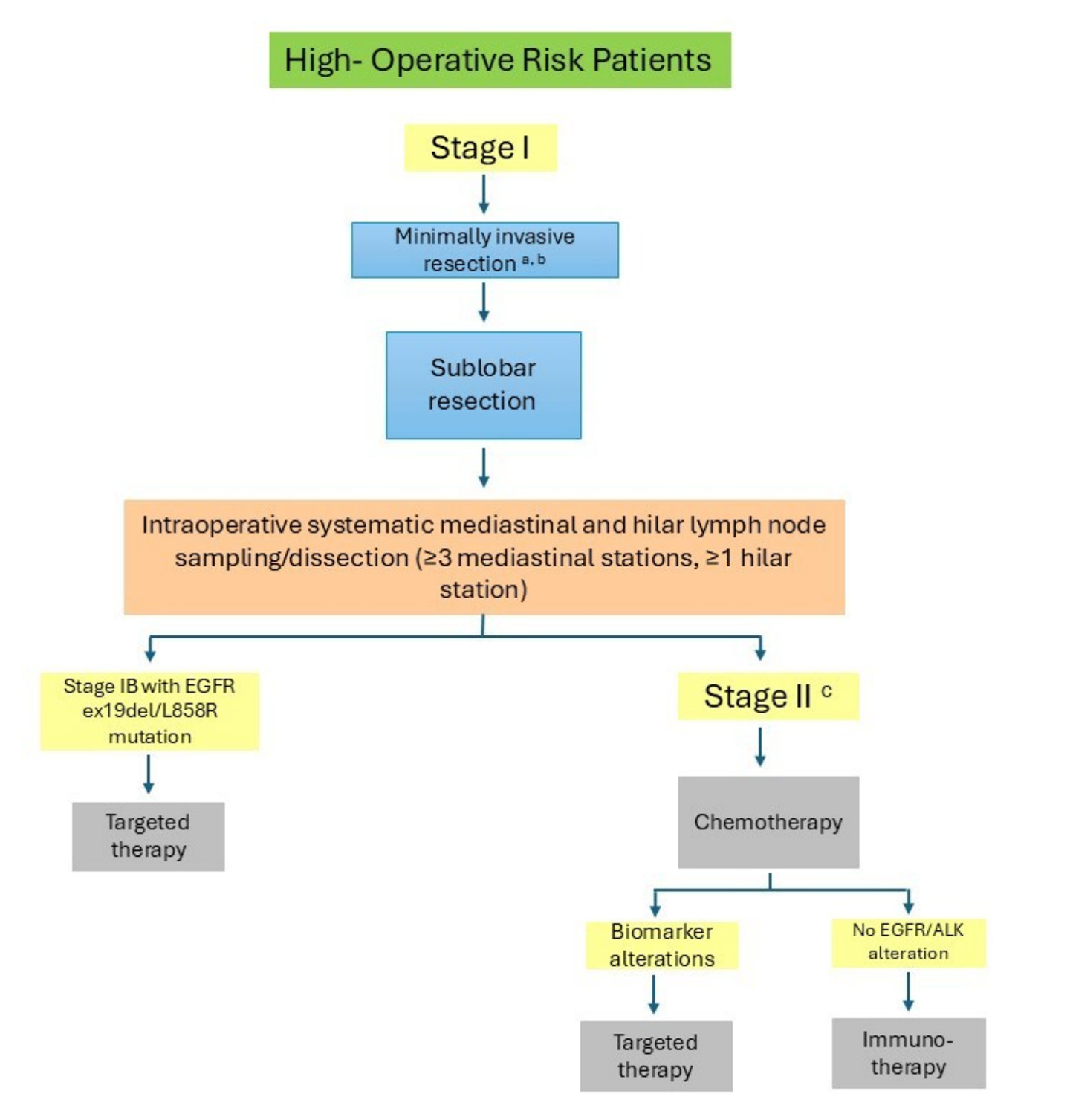 Figure 2 Sample management algorithm for high-operative risk patients.
Figure 2 Sample management algorithm for high-operative risk patients.
A. Resection suggested over stereotactic body radiotherapy or ablative techniques.
B. Resection by a board-certified thoracic surgeon suggested.
C. Based on upstaging.
ALK = anaplastic lymphoma kinase; EGFR = epidermal growth factor receptor
Figure 3 Sample management algorithm for medically inoperable patients. SBRT = stereotactic body radiotherapy.